AAC in Adults with Acquired Communication Impairments
This is a curated collection of information and resources related to supporting augmentative and alternative communication (AAC) with adults with acquired communication impairments. We encourage you to explore and judge for yourself which to add to your toolbox.
These resources are for educational purposes. This is not an exhaustive list. Inclusion does not signify endorsement. Use of any information provided on this website is at your own risk, for which NWACS shall not be held liable.
Do you have a favorite resource or strategy that we missed? Send us an email to share!
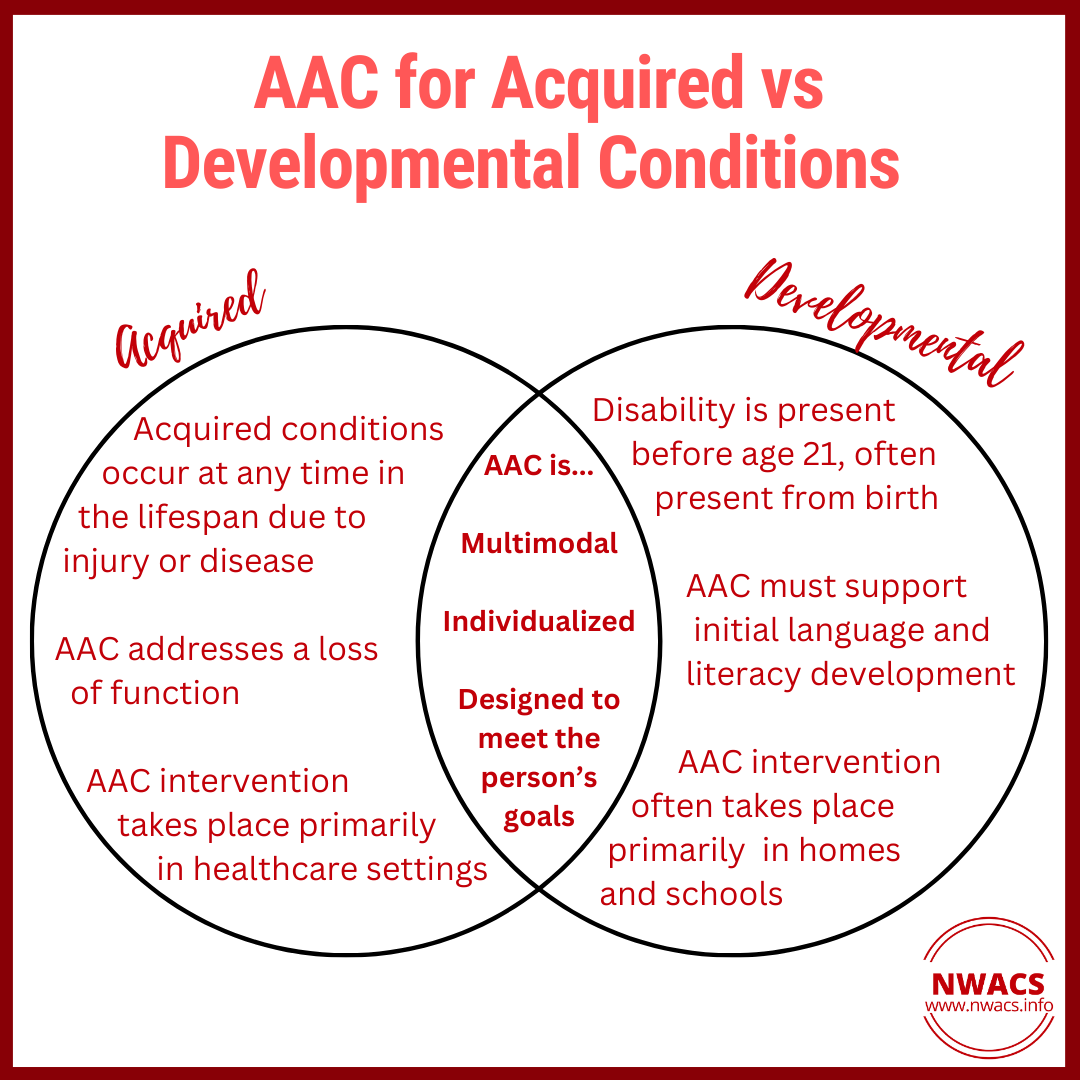
NOTE: The term “acquired communication impairments” covers many conditions and disabilities. Acquired communication impairments occur due to an injury or medical condition. For example, they may be due to a traumatic brain injury or stroke. They may also be due to a degenerative condition such as dementia or ALS. They differ from intellectual and developmental disabilities (IDD). IDD emerges in childhood and is often present from birth. Acquired conditions may affect speech, language, and/or cognition.
Examples include:
Aphasia: an impairment in language skills. Aphasia can affect a person’s ability to
express themselves
understand others
read
write
Motor speech disorders (MSDs): impairments in speech production that result from brain damage. MSDs include dysarthria and acquired apraxia of speech. These conditions can impact
speech clarity
naturalness
efficiency
Cognitive-communication impairments: communication disabilities due to impairments in cognition. For example, a person with dementia may have difficulty communicating due to impairments in attention and memory.
Common causes of acquired communication impairments include:
Vascular conditions (e.g., stroke)
Neoplastic conditions (e.g., a brain tumor)
Traumatic brain injury (TBI) or spinal cord injury (SCI)
Degenerative conditions (e.g., ALS, multiple sclerosis, Parkinson’s disease, Huntington’s disease, dementia)
What does supporting communication look like for adults with acquired communication impairments?
Every person with an acquired communication impairment is different. Supporting communication can take shape in many different ways. It must account for the person’s specific strengths, difficulties, and needs. A few considerations are outlined below.
AAC interventions can look different depending on the medical setting.
Acute care hospital: Patients with sudden injuries such as stroke or TBI are often seen first in this setting. AAC focuses on immediate communication needs during the early stages of acquired brain injury. At this stage, no-tech and light-tech AAC are often emphasized. Common goals in this setting include:
evaluating speech, language, and cognition to diagnose impairments
providing education to patients and families
optimizing the patient’s ability to communicate wants/needs and participate in their medical care
Inpatient rehabilitation / post-acute care: With targeted intervention, the brain can often recover a lot of function in the first few weeks to months after an injury (a concept called neuroplasticity). Intervention at this stage is often heavily focused on restoring function in speech, language, and cognition. For more severe impairments, intervention may also emphasize compensation with AAC.
Outpatient therapy: This setting tends to involve the most robust AAC evaluation and intervention processes.
High-tech AAC is most readily targeted in this setting, although it can be introduced earlier. For those with conditions such as stroke and TBI, impairments are often more stable at this time. AAC can be used to supplement or elaborate on spoken communication. It can also be used more as an alternative to spoken communication. The types of AAC used and the manner in which AAC is utilized may change over time.
Patients with progressive and degenerative conditions are often seen first in the outpatient setting. For these patients, intervention with AAC focuses on planning for the future since a loss of function is expected.
AAC interventions can vary considerably based on the type of acquired condition being treated.
Some conditions are stable or expected to improve. People with these conditions may rely on AAC less as time goes on. They are introduced to AAC because they have experienced a sudden loss of function. Sometimes, they may only need AAC interventions in the short term.
Degenerative conditions are associated with a progressive loss of function. People with these conditions often need to rely on AAC and other assistive technology more as time goes on. They often must start thinking about AAC before they actually need it. The person and their care team must plan for anticipated communication changes that will arise in the future. The AAC system must be adapted over time as their needs change.




Dynamic AAC systems are a must!
Consider the following examples:
A person who has just experienced a stroke may have significant impairments in speech and language. But, they gradually regain some of their function over time. This can occur over days, weeks, months, and even years. This person may need robust AAC support primarily as an “alternative” to speech early in the recovery process. Later on, they may only need AAC in certain contexts to “augment” their oral speech.
A person with ALS will experience a progressive loss of function over time. This can impact speech, breathing, and body movement. Early in the disease process, their oral speech may be enough for communication. They eventually transition to an AAC device with eye gaze technology as they experience a loss of motor function in their speech and body muscles. Late in the disease process, they may rely on partner-assisted scanning for most communication interactions.
A person in the early stages of dementia may be able to communicate quite well. During this time, an SLP might work with the person and their family to develop communication supports. These supports might not be immediately necessary, but they can support long-term communication.
Key Goals

addressing a loss of function (rather than communication development)
grief can play a large role in AAC acceptance and use
intervention often involves a significant amount of counseling
supporting participation in meaningful activities and social roles
family roles (spouse, parent, grandparent, etc.)
social connection
work / career
community involvement
hobbies and interests
supporting communication across a wide variety of environments / contexts
compensating for declining function in those with degenerative conditions
meeting the person where they are now, while also planning for the future
What AAC Looks Like
Many factors can impact a person’s ability to access, learn, and use AAC:
language impairments (e.g., aphasia)
motor speech impairments (e.g., dysarthria, apraxia of speech)
other motor impairments (e.g., paralysis, weakness, or incoordination of the muscles that control the hands, arms, legs, and/or eyes)
cognitive and/or behavioral impairments (e.g., right-hemisphere dysfunction, dementia). These may manifest in a variety of ways. For example, a person may experience:
reduced insight into impairments (and thus reduced understanding of purpose / need for AAC)
difficulty with attention and concentration
difficulty with memory and new learning
difficulty with executive functions (e.g., problem-solving, planning, organizing information, mental flexibility, self-monitoring)
behavioral changes (e.g., apathy, indifference, poor frustration tolerance, irritability)
brain fatigue associated with brain injury
other environmental factors
culture
home language(s)
social support (family, friends, community)
access to medical services
insurance
living situation
and more
With all these factors in mind, know that AAC can look very different between one person and the next - even if they are experiencing similar impairments.
AAC may include a wide variety of supports, such as the following:
No-tech: Showing the person that we communicate in many ways beyond speech.
capitalize on natural communication behaviors
facial expressions, gestures, etc.
Light-tech: There are many AAC options available that don’t require a high-tech speech-generating device. Some people may value more discrete AAC options, which are often captured here.
wallet cards to help someone quickly communicate their needs with new communication partners
use of writing to support communication
context-specific communication boards or cue cards
scripts to use when speaking on the phone or in other specific situations
small keychain flipbooks that can be used for self-cueing or quick communication
communication books or “memory books” for individuals with dementia
High-tech: Robust speech-generating devices (SGD) can be an appropriate choice for many people. Especially those with progressive conditions or more severe impairments from an injury. A few options / considerations may include:
Visual scene displays: VSDs use contextually rich, personally relevant photographs of activities and events to inspire conversational exchanges. VSDs have shown promise for people with dementia as well as those with aphasia. (Note: VSDs can be light or high tech)
Devices designed / organized specifically for people with aphasia. Organized into predictable categories and highly customizable. May focus on functional full-phrase messages rather than word-by-word message generation.
Some people may not be open to an SGD suggested by the clinician, but might be willing to try an iPhone app or something that feels more discrete / accessible. Meet the person where they are!
SGDs with options for alternative access, such as eye gaze or scanning. Some people with acquired conditions may have difficulty accessing a device due to impairments in body movements. Some people may need to use different access methods as their medical condition progresses over time.
Access to the internet, phone, social media, email, etc., can be an important feature to consider with high-tech devices.
Consider voice preservation options for people with ALS or other degenerative conditions: voice banking, message banking, and “double dipping”




Helpful Implementation Strategies
Counseling
Some people can be resistant to AAC. They have communicated using speech their whole lives and are now adjusting to a change in function. They may think AAC is “giving up” on restoring their speech and language function. They may feel that they don’t need AAC. Addressing grief, anger, and other difficult emotions is important when the idea of AAC is met with resistance. In these cases, it is important to meet the person where they are and bring those difficult emotions to the surface so they can be addressed.
It can be beneficial to gently introduce AAC concepts with simple no-tech options or discrete light-tech supports. It is important to show how AAC is just one tool that can be used to meet the person’s goals. And AAC does not mean giving up on spoken communication. In fact, AAC can even be used to improve spoken language!
Incorporating communication partners during assessment and intervention
Many people with acquired impairments will benefit from some level of communication partner support to learn or use AAC.
Achieving input and buy-in from communication partners can sometimes support AAC acceptance and use. In turn, this ultimately supports communication success and quality of life.
Multimodal communication
Capitalize on preserved abilities and natural communicative behaviors.
Focus on the individual’s goals. If they want to focus primarily on improving their spoken communication, that is okay! Use of AAC to communicate more effectively in the “here and now” does not prevent treatment focused on rehabilitating speech and language.
Explore options! It can be less daunting to start with simple, light-tech supports to facilitate openness to AAC rather than immediately diving into high-tech AAC.
AAC may not need to be used 100% of the time. An AAC app or device can be used to help someone practice their speech or cue themselves for elaboration. They may only need to use AAC in certain situations. Remember that AAC is highly customizable and adaptable. It isn’t “all-or-nothing”.
Resources to Explore

Articles, Books, and Documents
Augmentative and Alternative Communication: Challenges and Solutions (2021), Billy Ogletree
Chapter 6: AAC Interventions in Persons with Aphasia by Tiffany Chavers, Cissy Cheng, and Rajinder Koul
Chapter 7: Decision-Making for Access to AAC Technologies in Late State ALS by Deirdre McLaughlin, Betts Peters, Kendra McInturf, Brandon Eddy, Michelle Kinsella, Aimee Mooney, Trinity Deibert, Kerry Montgomery, and Melanie Fried-Oken
Chapter 8: Access to AAC for Individuals with Acquired Conditions: Challenges and Solutions in Early Recovery by Susan Koch Fager, Jessica Gormley, and Tabitha Sorenson
Augmentative and Alternative Communication: Engagement and Participation (2017) by Erna Alant
Chapter 9: Engagement, Participation, and People with Severe Dementia
Fundamentals of AAC: A Case-Based Approach to Enhancing Communication (2023), Nerissa Hall, Jenifer Juengling-Sudkamp, Michelle L. Gutmann, and Ellen R. Cohn (eds)
Supporting Communication for Adults with Acute and Chronic Aphasia (2013), Nina Simmons-Mackie, Julia King Fischer, and David R. Beukelman (eds)

Materials
Widgit Health: free healthcare & emergency communication boards, including bedside message boards and medical encounter boards in multiple languages


Webinar Recordings
AAC in the Cloud presentation recordings
AAC Device Personalization for Adults with Aphasia by Amanda Gunn & Caitlin Mueller (2020)
AAC in the Workplace by D. Burrow (2019)
Powerful Insights from Adult AAC Users That Challenge How We Practice AAC by Amanda Hartmann (2019)
Lingraphica Learning Portal - free live and recorded webinars
NWACS Evening Seminar recordings
AAC Assessment Considerations in Degenerative Disease (9/28/23)
AAC Goal Setting 101 (10/26/23)

Other Resources
OCALI Assistive Technology Internet Modules - AT for Adults and Adults with DD
Useful Tips
Counseling in Communication Disorders - Resources for SLPs:
Holland, A. L., & Nelson, R. L. (2013). Counseling in communication disorders: A wellness perspective. Plural Publishing.
McFarlane, L. (2012). Motivational interviewing: Practical strategies for speech-language pathologists and audiologists. Canadian Journal of Speech-Language Pathology and Audiology, 36(1), 8-16.
Lanzi, A. M., Ellison, J. M., & Cohen, M. L. (2021). The “Counseling+” Roles of the Speech-Language Pathologist Serving Older Adults With Mild Cognitive Impairment and Dementia From Alzheimer’s Disease. 6, 987–1002.
Turner-Stokes, L., Kalmus, M., Hirani, D., & Clegg, F. (2005). The Depression Intensity Scale Circles (DISCs): A first evaluation of a simple assessment tool for depression in the context of brain injury. Journal of Neurology, Neurosurgery and Psychiatry, 76(9), 1273–1278. https://doi.org/10.1136/jnnp.2004.050096
Ackerman, S. J., & Hilsenroth, M. J. (2001). A review of therapist characteristics and techniques positively impacting the therapeutic alliance. Clinical Psychology Review, 23, 1–33.
Riley, J. (2002). Counseling: An approach for Speech-Language Pathologists. Contemporary Issues in Communication Sciences and Disorders, 29, 6-16.
Selected References:
Baxter, S., Enderby, P., Evans, P., & Judge, S. (2011). Barriers and facilitators to the use of high-technology augmentative and alternative communication devices: A systematic review and qualitative synthesis. International Journal of Language and Communication Disorders, 47(2), 115-129. https://doi.org/10.1111/j.1460-6984.2011.00090.x
Beukelman, D.R., Fager, S. K., Ball, L., & Dietz, A. (2007). AAC for adults with acquired neurological conditions: A review. Augmentative and Alternative Communication, 23(3), 230-242. https://doi.org/10.1080/07434610701553668
Beukelman, D., Fager, S., & Nordness, A. (2011). Communication support for people with ALS. Neurology Research International, 2011. https://doi.org/10.1155/2011/714693
Blake, D. J., & Bodine, C. (2002). An overview of assistive technology for persons with multiple sclerosis. Journal of Rehabilitation Research and Development, 39(2), 299-312.
Crema, C. (2009). Augmentative and Alternative Communication in the Geriatric Population: A Review of Literature. Perspectives on Gerontology, 14(2), 42–46. https://doi.org/10.1044/gero14.2.42
Hanson, E. K. & Fager, S. K. (2017). Communication supports for people with motor speech disorders. Topics in Language Disorders, 37(4), 375-388. https://doi.org/10.1097/TLD.0000000000000137
Koch Fager, S. (2018). Alternative access for adults who rely on augmentative and alternative communication. Perspectives of the ASHA Special Interest Groups, 3(12), 6–12. https://doi.org/10.1044/persp3.sig12.6
Peters, B., O’Brien, K., & Fried-Oken, M. (2022). A recent survey of augmentative and alternative communication use and service delivery experiences of people with amyotrophic lateral sclerosis in the United States. Disability and Rehabilitation: Assistive Technology, 0(0), 1–14. https://doi.org/10.1080/17483107.2022.2149866
Taylor, S., Wallace, S. J., & Wallace, S. E. (2019). High-technology augmentative and alternative communication in poststroke aphasia: a review of the factors that contribute to successful augmentative and alternative communication use. Perspectives of the ASHA Special Interest Groups, 4, 464-473. https://doi.org/10.1044/2019_PERS-SIG2-2018-0016





